Cancer-curing gene therapies present unique manufacturing challenges
Eric Olson | February 28, 2019 CliniMACS Prodigy is a closed platform that enables GMP-compliant automated cell manufacturing. Source: Miltenyi Biotec
CliniMACS Prodigy is a closed platform that enables GMP-compliant automated cell manufacturing. Source: Miltenyi Biotec
Conventional drug therapy combats disease by mass producing a single chemical substance that is effective for most patients with the disease. This line of attack is conducive to mass manufacturing of the drug on a large scale.
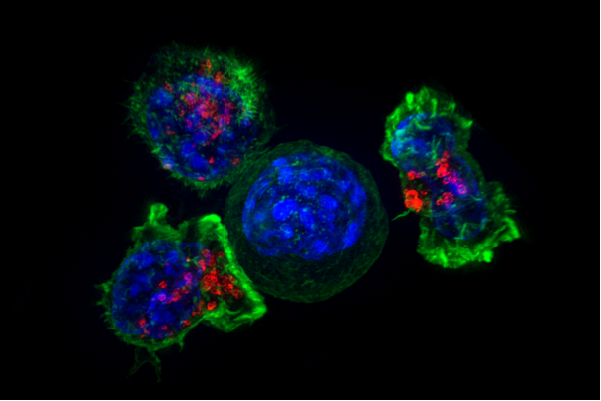 A high-resolution image of killer T-cells surrounding a cancer cell. In adoptive immunotherapies, a patient’s immune system is reprogrammed to destroy cancer cells. Source: National Institutes of Health
A high-resolution image of killer T-cells surrounding a cancer cell. In adoptive immunotherapies, a patient’s immune system is reprogrammed to destroy cancer cells. Source: National Institutes of Health
New adoptive cellular immunotherapies require a different approach to manufacturing. These therapies employ a patient’s own immune cells to eliminate disease. As a result, the pharmaceutical product must be tailored to each individual patient. The manufacturing process to enable this is necessarily different than that used for traditional drugs like cholesterol-lowering Crestor or rheumatoid-arthritis-fighting Enbrel.
New adoptive immunotherapies are currently being used to treat a relatively small number of patients. To scale the therapies to a much larger patient population, a number of manufacturing hurdles will need to be overcome.
Much of the current production for these therapies is manual work in which contaminants can enter the process and results may vary between technicians. Expanded production will be enabled by closed systems to reduce contamination risks, automated operations to increase efficiency, and closer process control to improve quality.
The effort may be well worth the cost. Adoptive immunotherapies are proving to be incredibly successful. In a clinical trial, 83% of 63 patients who were administered Novartis’ leukemia treatment Kymriah displayed complete remission after 3 months.
Adoptive immunotherapy workflow
Kymriah was the first treatment involving a gene therapy step to receive FDA approval in August 2017. The treatment is a type of adoptive immunotherapy known as Chimeric Antigen Receptor (CAR)-based T-cell therapy, in which the patient’s own immune cells – specifically, a type of white blood cells called T-cells – are engineered to recognize and hunt down cancer cells.
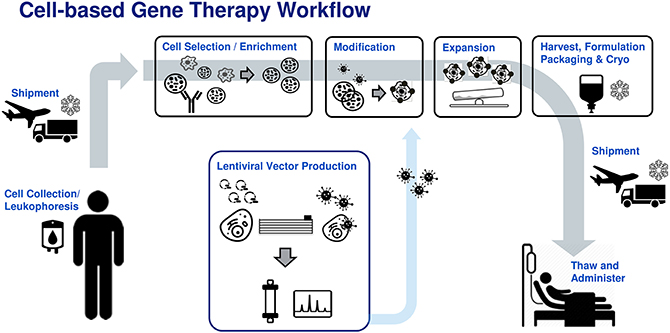 Typical workflow for adoptive immunotherapies. Source: Iyer, Bowles, Kim and Dulgar-Tulloch
Typical workflow for adoptive immunotherapies. Source: Iyer, Bowles, Kim and Dulgar-Tulloch
The production process for Kymriah is typical of adoptive immunotherapies in general and can be summarized as follows. First, T-cells are collected from the patient by filtering their blood in a process known as leukapheresis. The T-cells are then activated and genetically engineered in a process called transduction, in which genes are inserted into the T-cell with the help of a virus to reprogram them to hunt cancer cells.
Next, the number of existing lymphocytes in the patient is reduced through chemotherapy. Finally, the engineered T-cells are injected into the patient. These CAR-T cells will target antigens on cancer cells, bind to them, activate, proliferate and become cytotoxic to the cancer cells to destroy them.
Manufacturing challenges
Since each patient receives personalized, modified immune cells, the manufacturing process for adoptive immunotherapies has unique challenges that are not present in the production of conventional drugs. As the treatments transition from clinical trials to commercial treatments, manufacturing operations will need to be optimized.
One issue concerns the reagents used in the manufacture of cell therapies. Undefined reagents – such as serum or culture media used for cell expansion – pose safety risks to patients due to varying compositions from batch to batch and contamination risks. To improve patient safety, reagents should ideally be chemically defined (CD) to conform to precise definitions identifying the exact concentrations of all their components and be free of any components derived from human or non-human animals.
Reagents should also be produced according to good manufacturing practices (GMP) to prevent harm to patients. GMP-grade products are made by trained personnel following documented procedures within a quality management system. Complying with GMP guidelines ensures batch-to-batch consistency of composition and quality.
Selection of cells
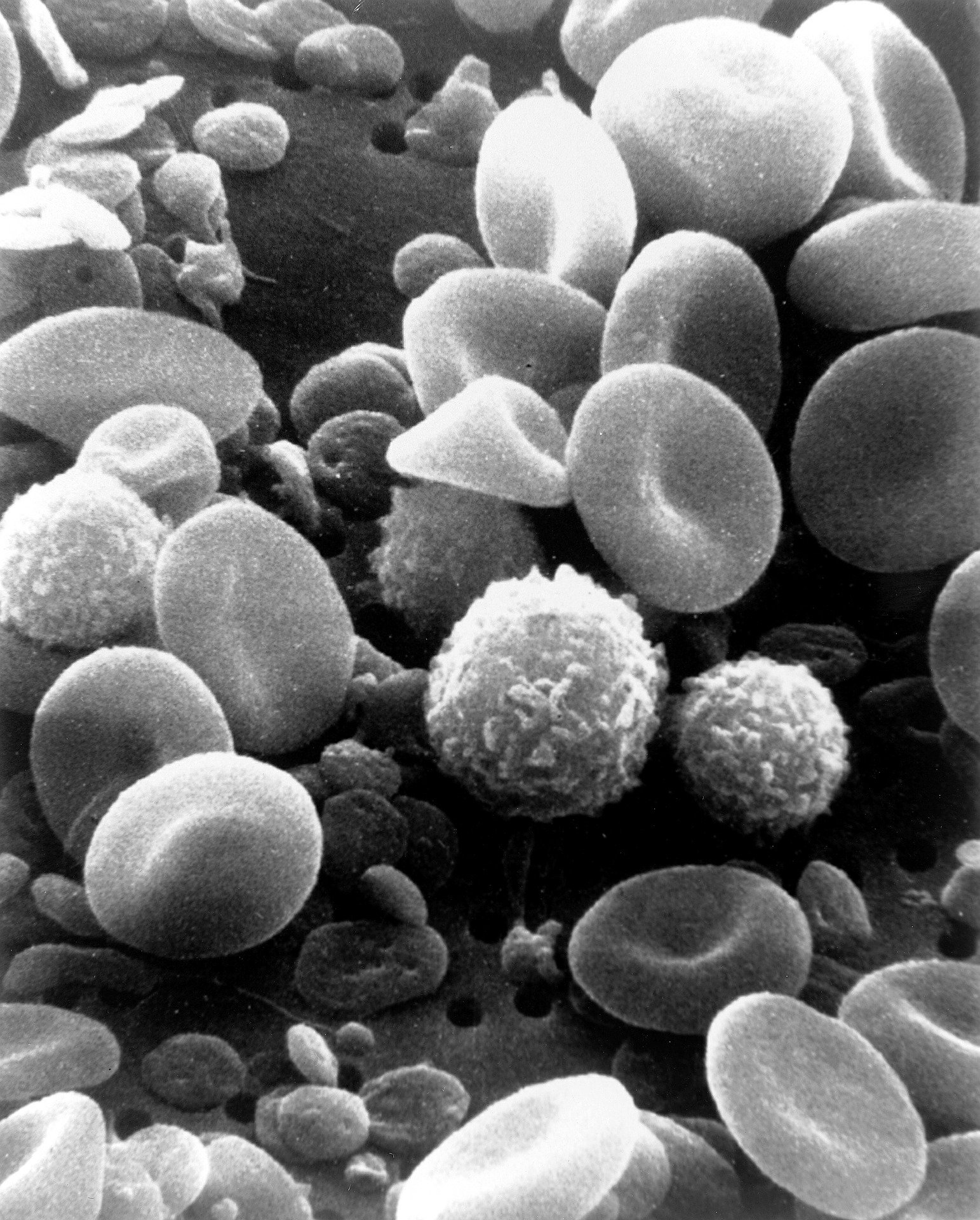 A scanning electron microscope image of human blood showing its various components including red blood cells, white blood cells and platelets. Leukapheresis is the process by which a patient’s immune cells are separated from the other components of blood. Source: National Cancer Institute
A scanning electron microscope image of human blood showing its various components including red blood cells, white blood cells and platelets. Leukapheresis is the process by which a patient’s immune cells are separated from the other components of blood. Source: National Cancer Institute
The first step in the production process of typical adoptive immunotherapies involves isolating the patient’s immune cells that will be modified. A few different types of equipment exist for this purpose, each with its own pros and cons.
Density gradient separation systems can separate cells through centrifugation based on size but aren’t able to differentiate between cells of comparable size, such as healthy T cells and leukemia cells.
Other techniques separate cells based on cell surface markers that are specific to certain antibodies. The antibodies are conjugated (combined) with a molecule that can be used to separate the cells.
In Fluorescence-Activated Cell Sorting (FACS), the antibodies are conjugated with fluorochromes and the cells are separated one-at-a-time based on their fluorescence. FACS is a slow process, so separation of a complete leukapheresis batch takes hours even with the newest equipment.
Magnetic-Activated Cell Sorting (MACS) uses antibodies conjugated to magnetic beads to discriminate between cell types. Although MACS is faster than FACS, early MACS techniques could not separate the magnetic beads from cells after classification, which is not ideal for immunotherapy applications in which cells are injected into patients. The newest MACS techniques, however, solve this issue.
Decreasing the time it takes to complete the cell selection process and thus reducing the cost of the operation will be achieved by advances in our understanding of cell and conjugation chemistries and the development of processes and equipment with improved selection specificity.
Cell activation
After the correct immune cells have been isolated from the patient’s other blood components, they must be activated. Antigen Presenting Cells (APCs) are often used for the activation process, although there are a few challenging aspects of this method that will need to be addressed to enable adoptive immunotherapy manufacturing on a wider scale.
First, APCs are harvested from the patient’s own blood, so very ill patients might have too few of the cells in their system for the process to be effective. In addition, there may be variation among patients in terms of the ability of their APCs to activate immune cells. Furthermore, producing APCs to GMP standards has substantial cost considerations.
Transduction
 CRISPR/Cas9 – a gene-editing technique that cuts out targeted pieces of a cell’s DNA and replaces them with a customized DNA sequence – shows potential as a future method to reduce the costs associated with modifying immune cells in adoptive immunotherapies. Source: National Institutes of Health
CRISPR/Cas9 – a gene-editing technique that cuts out targeted pieces of a cell’s DNA and replaces them with a customized DNA sequence – shows potential as a future method to reduce the costs associated with modifying immune cells in adoptive immunotherapies. Source: National Institutes of Health
Following activation of the immune cells, their genetic code is modified so that they become cancer hunters in a process known as transduction. This process employs viral vectors to deliver the modified gene to immune cells. The issue here is that viral vectors – derived from pathogens – are quite costly to produce as a result of testing requirements to ensure their safety.
Improving the efficiency of viral vector production at scale or finding an alternative method to carry out genetic modification of the immune cells would reduce the costs of adoptive immunotherapy manufacturing. One promising avenue lies in harnessing the CRISPR/Cas9 method to execute gene edits.
Cell expansion
Once the patient’s immune cells have been modified, this population of cancer-killing cells must be multiplied in a process known as cell expansion. There are a few different tools to accomplish this task.
Gas permeable bags and G-Rex bioreactors allow for the efficient transfer of gas to the cells during expansion, are simple to set up, and are cost-effective at small scales. These two tools, however, lack automation and in-process monitoring, so they are not ideal for large-scale production.
Wave-mixed bioreactors, another tool, are closed systems with integral automation functions to lower the manual work involved in cell expansion. They typically, however, have minimum starting volumes, requiring initial seeding to reach the necessary quantity before wave-mixed bioreactors can be used.
All-in-one solutions like the CliniMACS Prodigy are capable of completing several steps in the immunotherapy production process in one machine, including cell selection, expansion, washing and final product formulation. Combining multiple tasks in one piece of equipment improves convenience and decreases the risk of contamination, but may reduce the overall efficiency of a commercial immunotherapy manufacturing operation.
 Pre-installed automated manufacturing steps on the CliniMACS Prodigy cell factory. Source: Miltenyi Biotec. (Click to enlarge.)
Pre-installed automated manufacturing steps on the CliniMACS Prodigy cell factory. Source: Miltenyi Biotec. (Click to enlarge.)
For example, the instrument must complete its serial operations in order. After completing cell selection operations on a specific patient’s cell line, the tool would be unavailable to start cell selection on another patient’s cell line until it completed the expansion, washing and formulation steps. Splitting up these operations between separate machines could improve overall manufacturing efficiency for a plant producing cells for multiple patients.
In-line process analytics
To scale adoptive immunotherapies from small clinical trials to broader commercial operations, critical quality attributes (CQAs) of the cell product will need to be continuously monitored. Sampling for process values like cell viability, density and metabolites – often performed manually – will need to transition to automated measurement systems.
Ideally, in-line process analytical technologies (PATs) will enable an automated monitoring and feedback loop to measure process values and adjust process operations autonomously for delivery of a high-quality final product.
Downstream processing
The final steps of the adoptive immunotherapy manufacturing process include collecting and concentrating the cultured cells, washing away culture media and replacing it with a formulation buffer, and freezing the product in cryobags to be thawed before infusing the patient. Closed, automated equipment for some of these steps exist. Moving the product from one unit operation to the next, however, can present integration challenges, especially if the equipment and consumables are made by different companies.
Scaling production
As adoptive immunotherapies graduate from research trials to commercial treatments, manufacturing processes will need to scale out to improve quality, boost yields, reduce costs and expand patient access. Advancements in equipment capacity, single-use consumables, sensors, system integration and automation will enable this life-saving therapy to reach a wider pool of patients.
Further reading
Iyer RK, Bowles PA, Kim H and Dulgar-Tulloch A (2018) Industrializing Autologous Adoptive Immunotherapies: Manufacturing Advances and Challenges. Front. Med. 5:150. doi: 10.3389/fmed.2018.00150
Discover more on Engineering360
Find lab equipment and scientific instruments including lab automation tools, sample preparation and liquid handling products, lab supplies and other lab equipment.